Category: Healthcare Insights

Advances in Practice: Implementing the IDDSI
Published by Feeding Matters on May 01, 2019
 From 2013 through 2014, the IDDSI engaged in international systematic review and solicitation of stakeholder input, which included health professions, patients and caregivers, industry and researchers. The results? In 2015, the IDDSI panel ultimately created standardized guidelines for describing and determining food and liquid consistency. The IDDSI classification has eight levels, 0 through 7. A simple timed measure of the gravity flow rate from a 10ml syringe is used to classify liquids. The IDDSI website provides free, open access instructions with training videos on how to classify liquids based on this testing method.
Families and professionals alike now have access to shared terminology and an easy cost-effective and reliable method of determining food and liquid consistency. Visit the IDDSI website for downloadable handouts, instructions, and videos on how to implement the internationally endorsed IDDSI. The Academy of Nutrition and Dietetics also offers an IDDSI Boot Camp, including a monthly step-by-step plan for implementing the IDDSI in your workplace or community.
From 2013 through 2014, the IDDSI engaged in international systematic review and solicitation of stakeholder input, which included health professions, patients and caregivers, industry and researchers. The results? In 2015, the IDDSI panel ultimately created standardized guidelines for describing and determining food and liquid consistency. The IDDSI classification has eight levels, 0 through 7. A simple timed measure of the gravity flow rate from a 10ml syringe is used to classify liquids. The IDDSI website provides free, open access instructions with training videos on how to classify liquids based on this testing method.
Families and professionals alike now have access to shared terminology and an easy cost-effective and reliable method of determining food and liquid consistency. Visit the IDDSI website for downloadable handouts, instructions, and videos on how to implement the internationally endorsed IDDSI. The Academy of Nutrition and Dietetics also offers an IDDSI Boot Camp, including a monthly step-by-step plan for implementing the IDDSI in your workplace or community. 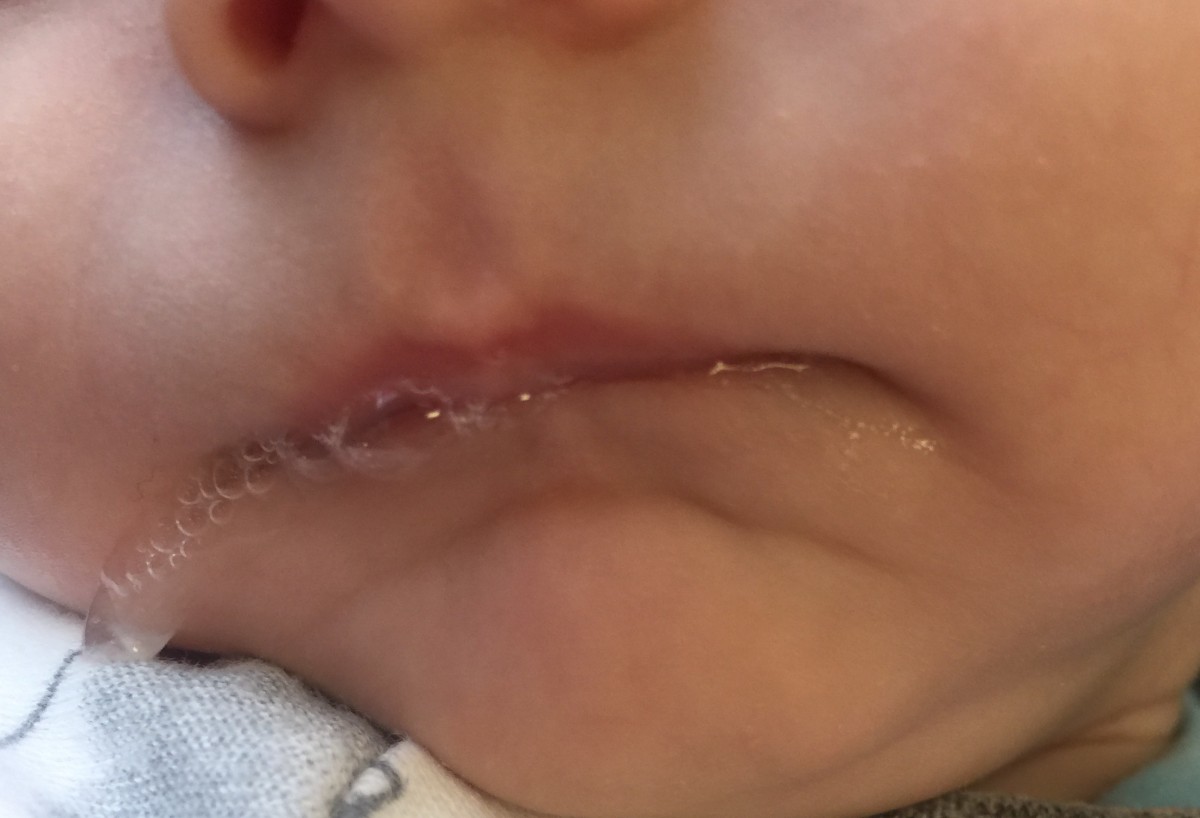
Feeding Infants with Recessed Jaw or Retrognathia at Breast or with Bottle
Published by Allyson Goodwyn-Craine on Jun 10, 2017
Infants with recessed jaw/ retrognathia present with unique feeding challenges and are sometimes misdiagnosed with ankyloglossia or tongue tie. This is of particular concern, because in some cases a frenulectomy is contraindicated. Although the anterior maxillary and mandible alignment is impacted, the primary concern is the tongue sitting posteriorly toward the pharynx. In severe cases airway obstruction can occur but milder cases also require consideration for airway patency. These babes often present with stridor reflective of increased respiratory effort but when paired with a confirmed diagnosis of laryngeal or tracheal malacia adequate respiratory support needed for sustained energy and coordination for feeding are frequently compromised.
The discrepancy between the maxilla and mandible often cause the nipple and areola to compress with anterior rotation. The position of the tongue can also inhibit elevation and retraction of the posterior tongue needed to recreate adequate inner oral pressure during the suck needed to efficiently draw milk from the breast. These oral mechanics can cause irritation to the nipple or tissue trauma or they have difficulty transitioning off of nipple shields sometimes mistaken as characteristic of ankyloglossia (tongue-tie). Many babes have improved latch in this position as gravity assists with tongue and occasionally jaw forward.
Detection of a recessed jaw can be a bit challenging. Infants naturally have a slightly recessed chin/jaw as part of normal development; however, those that present with a gap of 3 mm or more between the anterior upper and lower gum line often struggle at breast. These infants sometimes have prominent chins with a horizonal crease between the mental region and the lower lip. The lower lip often rests tucked behind the upper lip or superior alveolar ridge. Observation at breast and bottle will also reveal increased facial tension particularly along the lateral orbicularis oris often resulting in a narrow latch as the babe tries to compensate for anterior rotation of the nipple between the upper and lower gum lines. In more involved cases the infant struggles with the extension reflex of the tongue needed for latch stability as gravity pulls the back of the tongue posteriorially.
The good news is that positioning adjustments have proven very helpful, particularly at breast to use gravity to move the tongue anteriorly in the mouth creating additional pharyngeal space. For babies without sternal precautions or poor respiratory endurance I suggest a trial with Mom reclined with babe in prone position (also known as tummy to tummy, laid back or biological position). I find most success with placing a rolled bath towel or narrow end of the Gia or breast feeding pillow at babe’s chest allow them to come down onto the nipple without head extension. The breastfeeding pillow can also provide support through the baby’s hips as they rest in a tucked position in the center of the pillow with the lower inside edge supporting their bottom. It is not uncommon to hear less stridor in this position as a result.
For bottle feeding, elevated side lying with slight anterior rotation at the hips) or high cradle (with hips slightly forward, not directly under the shoulders) can work nicely. These positions also provide nice support for respiration. I personally prefer placing babe in classic football hold but rotate their hips and shoulders so they are “stacked” which also places the babe at a nice angle with space for the bottle and supports lots of yummy eye contact/engagement.
When bottle supplementation is needed, the Playtex Drop In Nurser with the Natural Latch nipple provides nice support along the jaw when the bottle is held at a slight angle to allow the lower edge of the nipple along the lower lip. I typically prefer this bottle/nipple for breast feeding infants to match the gape/latch that compliments oral positioning at the breast. Infants with small gaps between the maxilla and mandible typically show no concerns for breathing. However, infants with wide gaps require careful monitoring. If an infant demonstrates any stress responses in supine, parents report concern for potentially obstructive noises during sleep or the young infant spontaneously moves themselves from their back to side lying a sleep study and/or airway patency assessment should be done by an otolaryngologist (ENT). The infant’s pediatrician needs to be aware of these concerns for consideration of positioning for sleep.Some pediatricians may consider elevated or side lying sleep positioners specifically designed for these purposes. These should only be used under the direction of the physician.
The majority of infants with a slightly recessed jaw outgrow these feeding concerns. At around 3-4 months of age the infant’s neck elongates and the pharynx deepens as the jaw moves forward with facial growth. This brings the posterior tongue slightly forward with increased space allowing for functional tongue elevation and retraction. At this point most infants can transition to more traditional breastfeeding positions.
About Allyson Goodwyn-Craine
 Allyson Goodwyn-Craine (Ally) began her career in 1989. She is a Neuro-Developmental Treatment (NDT) trained Pediatric Speech-Language Pathologist/Feeding Specialist who has worked in Private Practice, Shriner’s Children’s Hospital, Randall Children’s Hospital, and now at Kaiser Sunnyside Medical Center. Ally enjoys helping medically complex babies and toddlers who struggle with feeding challenges from breast, bottle, and tube feedings to transitioning to solid foods. Ally joins infants, toddlers, and their parents in the NICU, NICU Follow-Up Clinic, outpatient treatment, and as a member of the Cleft Palate team.
Allyson Goodwyn-Craine (Ally) began her career in 1989. She is a Neuro-Developmental Treatment (NDT) trained Pediatric Speech-Language Pathologist/Feeding Specialist who has worked in Private Practice, Shriner’s Children’s Hospital, Randall Children’s Hospital, and now at Kaiser Sunnyside Medical Center. Ally enjoys helping medically complex babies and toddlers who struggle with feeding challenges from breast, bottle, and tube feedings to transitioning to solid foods. Ally joins infants, toddlers, and their parents in the NICU, NICU Follow-Up Clinic, outpatient treatment, and as a member of the Cleft Palate team.
Allyson served on the Financial Planning Board of the American Speech-Language-Hearing Association. She is a past president of the Oregon Speech-Language-Hearing Association. She has served on the advisory board and as an adjunct professor at Portland State University for 19 years and is a guest lecturer in Pacific University and University of Oregon graduate programs. She has also traveled nationally and taught as a member of the Education Resources clinical faculty. Allyson was recently awarded the Honors of the Association by the Oregon Speech-Language-Hearing Association.
Click here to contact Allyson
National Nutrition Month
Published by Feeding Matters on Mar 05, 2018
Every year, the Academy of Nutrition and Dietetics supports a nutrition education and information campaign called National Nutrition Month®. National Nutrition Month® encourages research through credible, scientific-based food and nutrition information. In addition, it inspires people to make sound food choices, as well as informed physical activity habits.
One of four domains in the coordinated care model encouraging a collaborative approach to pediatric feeding disorder, nutrition is the foundation for growth and development. Whether your child eats by mouth or through a feeding tube, good nutrition allows children to thrive. It directly affects a child’s brain activity and capabilities, fine and gross motor skill development, and overall health and wellness. Poor growth and nutrition for children can lead to lifelong issues and difficulties.
This year, the theme for National Nutrition Month® is “Go Further with Food.” This could mean preparing meals at home, choosing a healthy breakfast or simply picking snacks that are more nutritious. Often, adopting a healthier life style also means less food loss and waste.
That can be difficult for families navigating pediatric feeding disorder. Kristi Meyer, author of the children’s book The Adventures of Team Super Tubie and Professor at Cornell College in Iowa, considers a 504 medical plan meeting with her son’s school an important step. “In addition to the practical questions about who can replace our son’s g-tube if it were to fall out while at school, there are the emotional and social concerns that we, as parents, have in wanting our son to be accepted by his peers, never excluded from activities, yet proud of his differences.”
“In spite of all these concerns,” adds Kristi, “we have also learned there is something very comforting and reassuring about the opportunity to meet face-to-face with his teachers and school nurse whom he will get to know so well and rely on to be his support and safe haven throughout his hours away from home.”
For more information on nutrition and pediatric feeding disorder, visit feedingmatters.org/growth-nutrition.
KEEPING AN EYE ON YOUR CHILD’S OVERALL DEVELOPMENT
Published by First Things First on Mar 12, 2018
 If you are a parent or caregiver of a child 5 years old and younger, you can make a difference by monitoring your child’s physical, mental, social, and emotional development and talking about what you see with your son or daughter’s health care provider. This is not a way to find something “wrong” with your child, instead, it should be viewed as a partnership opportunity between families and healthcare providers to keep your child developing in the best way possible.
If you are a parent or caregiver of a child 5 years old and younger, you can make a difference by monitoring your child’s physical, mental, social, and emotional development and talking about what you see with your son or daughter’s health care provider. This is not a way to find something “wrong” with your child, instead, it should be viewed as a partnership opportunity between families and healthcare providers to keep your child developing in the best way possible.
- Keep notes and document issues that you are concerned about.
- Take pictures of your child doing a specific task.
- Record audios or videos on your phone of behaviors that concern you.
- Write down your questions and take them with you so you remember what to ask and tell your child’s primary care provider during your appointment.
- Call the toll-free, statewide Birth to 5 Helpline (1-877-705-5437). Nurses and child development experts are available to talk with you about your child, give you tips on which milestones they should have achieved for their age, and help you decide if a follow up with your health provider is needed.
- Fill out the online Ages and Stages Questionnaire from Easterseals. This free screening tool includes a series of questions regarding your child’s development and behavior. Results are emailed to parents within a couple of weeks and are intended to be used to follow up with a health provider regarding any identified issues.
- Complete the online Infant and Child Feeding Questionnaire from Feeding Matters. This free tool helps you better understand your child’s feeding habits and identify any areas of concern. Results can then be shared and discussed with your child’s physician. Additional resources for family support can be found on the Feeding Matters website.
- Contact Raising Special Kids if you have a developmental concern you want addressed, or if you think your child needs screening or further assessment.
- Get in touch with Child Find at your local school district for assistance with screening or special education services.
* * *
Feeding Matters and First Things First are united in supporting the health and wellbeing of Arizona’s children by nourishing a family-centered, comprehensive, and collaborative early childhood system. To learn more visit firstthingsfirst.org.
EMOJIS, IPADS AND G-TUBES, OH MY!
Published by Jennifer Wilson on Mar 14, 2018
This article is reposted with permission from The ASHA Leader Blog.
Have you ever tried to imagine feeding and swallowing treatment from a young child’s perspective? You might remember early negative feeding experiences making treatment challenging. You also might not fully understand concepts like “appetite” or “hunger.” Most likely, you also don’t really get why you work on feeding or what short- and long-term goals mean.
Working with young children who don’t comprehend why you’re there and what you’re helping them achieve can add another layer of complications to an already delicate process. Especially when transitioning from a gastrointestinal tube (g-tube) to oral feeding.
Feeding treatment can feel like a curvy, unpredictable path without mile markers. As the Tin Man, Dorothy and the Scarecrow head down the yellow brick road in the “Wizard of Oz,” they anticipate meeting “lions, tigers and bears.” Much like this tale down a tumultuous road, overarching fear and anxiety can often create an obstacle in providing feeding interventions.
I find helping clients understand the big-picture goal motivates them to continue down the path of feeding treatment, even when it seems scary or uncomfortable. I often turn to technology to communicate with clients and families. Easily accessible technology like sending photos or the universal meaning of emojis allows me to communicate these goals with my young clients quickly and clearly.
For example, a normal daily eating routine for many families involves grazing. Parents feed kids and themselves when schedules allow with no evident meal times. Talking about what having an appetite means and feels like, what a meal looks like, and which foods are proteins, carbohydrates, fruits and vegetables can help lay the groundwork for helping families understand and achieve goals. Next, I help clients and their families move toward healthy eating patterns. Communicating those concepts with the help of photos and emojis makes understanding more immediate and can more actively engage families.
Here are some strategies I use to help children feel more comfortable with new foods, provide tangible mile markers, and help the journey from g-tube intake to oral feeding go more smoothly.
- Create a social story to help the child understand why they come to feeding treatment. The social story could begin with pictures of the medical events leading to g-tube placement, the process of increasing oral intake at home and in treatment, and information about getting their tube removed when they reach a specific level.
- Create weekly goals for different types of protein, fruit/vegetable and carbohydrate intake. Challenge your client to text or email food emojis once they take tastes or have experiences with these foods.
- Help clients identify how their body feels before and after food experiences and when gastric discomfort should concern them. Work on increasing their ability to communicate discomfort and considering alternatives to spitting out or moving away from food using photos of smelling, licking or playing with food. Or how about an emoji sticking out its tongue? Providing visual supports can also help you create a gastric discomfort scale by assigning the numbers one through five to various images of people with stomach aches.
- Educate clients in ways they can “reset” when they feel overwhelmed. Help them identify calming strategies when their sensory system becomes overwhelmed. Offer them images of scenes they like, such as beaches, mountains, animals or other calming imagery. Send a short video of yourself taking deep breaths that they can mimic, or perhaps find a video or song they like so they can sing along or just listen.
- Give clients immediate and frequent feedback by recording sessions and playing moments of success. Continue to communicate the purpose and long-term goals of treatment during each session.
As our feeding/swallowing clients and caregivers become engaged team members, treatment can be an adventurous trip. Unlike lions, tigers and bears, emojis and iPads can provide comforting connectivity when managing the transition from g-tube to safe, oral feeding.
 Jennifer Wilson, MA, CCC-SLP, is a clinical instructor at the University of Tennessee Health Science Center. She has more than 20 years’ experience serving clients with pediatric dysphagia in a variety of settings. She is also a Feeding Matters Community Ambassador and an affiliate of the ASHA Special Interest Group 13, Swallowing and Swallowing Disorders.
Jennifer Wilson, MA, CCC-SLP, is a clinical instructor at the University of Tennessee Health Science Center. She has more than 20 years’ experience serving clients with pediatric dysphagia in a variety of settings. She is also a Feeding Matters Community Ambassador and an affiliate of the ASHA Special Interest Group 13, Swallowing and Swallowing Disorders.
STUDYING THE ECONOMIC BURDEN ON FAMILIES
Published by Feeding Matters on Apr 10, 2018
Over the years, Feeding Matters has witnessed many insured families spend hundreds, and sometimes thousands, of dollars out of pocket to cover non reimbursed costs related to their child’s pediatric feeding disorder. To fully and accurately capture the devastating financial burden related to pediatric feeding disorder, Feeding Matters began collecting data and testimonials from our families.
Determine the cost associated with out of pocket expenses for families. In order to further investigate the out of pocket expenses for families, Feeding Matters collaborated with FirstEval to create an Economic Impact Survey to collect data around the child and the family, including medical costs, supplies, lost income, child care, travel, education, time, parent/caregiver health, psychological impact, and demographic information related to pediatric feeding disorder. The results showed families are spending money on extra childcare, specialty foods, and travel to therapists to receive optimal care. This significant expenditure has drained many family’s bank accounts.
“We sold our home, moved to a rental house and ultimately had to file bankruptcy to be able to afford for me to work part time rather than full time and to afford my child’s weekly therapy visits. Even though I have a bachelors degree and professional career, I took a job as a nanny (making significantly less than I made previously) so that I could have the flexibility to take my child to therapy and to stay home with him when he was too sick to go to school. The pressure of trying to manage my full time job while he was sick and had so many appointments was simply too much for me.”Obtain data that will be used to help change the system of care and coverage around pediatric feeding disorder. The costs incurred by families navigating pediatric feeding disorder are not well understood by the reimbursement community and this has prevented them from being covered by most insurance companies. The data collected from the survey will be used to inform healthcare professionals and insurance companies of the financial burden of pediatric feeding disorder and influence the system changes that need to occur in order to obtain coverage for families. Feeding Matters is anxious to lead the way in helping families get the coverage they need.
It’s more than emotional stress that parents endure when their child has pediatric feeding disorder Money and finances continue to be top stressors for families managing pediatric feeding disorder. That stress, coupled with the emotional stress that families endure can be detrimental to one’s health. Families have indicated that they have heightened anxiety, difficulties in their relationship, and depression due to the financial stress of caring for a child with pediatric feeding disorder. When a parent is feeling these emotions, it is likely that their child will feel this too.
“I am killing myself trying to work full-time to support my daughter as a single parent. My parents had to move from out of state to help, and even with them here I am exhausted from trying to coordinate supplies, therapy, and her care while maintaining full-time employment. I want to quit and give up every day, but I can’t. It is maddening.”
Feeding Matters is currently looking at the findings and determining next steps for sharing this with the community.
Update: View more information here.
THE IMPORTANCE OF COLLABORATIVE CARE
Published by Feeding Matters on Apr 25, 2018
Every day, parents across the world struggle when their children are diagnosed with pediatric feeding disorder. Parents often feel helpless and it can be overwhelming to deal with questions like “which provider is best?”
“Feeding Matters has been such a big part of the feeding community. They have really done a great job advocating for families and creating resources for us as therapists and for families to really get a comprehensive look at PFDs,” says Amanda Hermann, a speech language pathologist. “Because each child’s feeding disorder will develop differently, you have to treat them all as an individual.”
Feeding Matters’ Coordinated Care Model examines the complexities of a child’s feeding disorder, focusing on the four key domains that significantly impact his or her lifelong well-being: medical, nutrition, feeding skill, and psychosocial.
- Medical: The act of eating is a complex task that involves the entire body and its organs working as one seamless unit. It takes 13 paired muscles (26 total) and six cranial nerves working in perfect harmony to move food and liquid from the mouth to the stomach. This process takes only seconds but is the single most complex and physically demanding task an infant will complete for the first few weeks, and even months, of life.
- Nutrition: Nutrition is the foundation for growth and development. Whether your infant or child eats by mouth or through a feeding tube, good nutrition allows children to thrive. It directly affects a child’s brain activity and capabilities, fine and gross motor skill development, and overall health and wellness.
- Feeding Skill: Learning to eat skillfully and comfortably is rooted in the development of sensory and movement skills that make it possible for an infant or child to suck, swallow, bite, and chew. Feeding skills and abilities include the social, communication, and interactive skills that integrate with mealtime skills.
- Psychosocial: When children are struggling to eat, behavior is their way of communicating that something may not be working the way it should. It is also how they show their like or dislike for certain food. These behaviors can often leave family members and caregivers feeling confused and frustrated, impacting the parent–child relationship and the child’s thoughts and behaviors toward feeding.
When correctly diagnosed, overcoming feeding disorders is possible. The true concern lies with early identification and intervention. Together through collaborative care and the proper support system, pediatric feeding disorder can become manageable and treatable.
5 FEEDING MATTERS’ VIRTUAL WORKSHOPS YOU CAN WATCH RIGHT NOW
Published by Feeding Matters on May 02, 2018
Feeding Matters is proud to offer families and professionals on-demand workshops through our online Knowledge Center. These workshops provide tips and tools on how to efficiently manage pediatric feeding disorder and other related, complex issues, including:
-
Common Feeding Hurdles in the Weeks and Months after Leaving the NICU
In this 60 minute virtual workshop, Dr. Pamela Dodrill, PhD, CCC-SLP, presents about what NICU families can expect when having a child who has pediatric feeding disorder. This workshop is for families who have children with pediatric feeding disorder and the healthcare professionals who care for them. Dr. Dodrill has specialized in working with infants and children with feeding disorders for over 15 years. Pamela has a number of publications in this area, regularly presents at international scientific conferences, and teaches courses and workshops on managing pediatric feeding problems for students and practicing health professionals.
-
Fostering Collaborative Care: Parent and Provider Perspectives
Listen to professionals from a feeding clinic talk about how the ICFQ can be used as an engagement tool to help identify potential pediatric feeding disorder and hear from a parent’s perspective on life after the NICU. From the provider perspective, Anais Cook, Caroline Duong and Dr. Andrew Chu join us from Texas Children’s Hospital Feeding Clinic. And with a very personal perspective, Ashley Collier participates in the conversation to discuss her journey with her daughter Macie, who was a 33 week preemie and struggled in the NICU to master suck/swallow/breathe.
-
Navigating the system: Coordinating Your Child’s Care
overwhelming, the appointments can be endless, and the medications numerous and constantly changing. Navigating your way through doctors, programs, food, medications, and medical procedures is usually left in the hands of the primary caregiver “the parent.” Shannon Goldwater has over 14 years of experience with her triplets. This workshop will provide tips and tools on how to efficiently manage your child’s complex needs.
-
Planting a Seed Towards Self-Care
In the event of an airplane emergency, one of the first rules they tell you to follow for your safety is to put your own oxygen mask on first before you assist anyone else. Because only when we help ourselves, do we have the ability to effectively help others. Often as caregivers this concept is difficult to practice. There is a mentality that you don’t have time to care for yourself and that your child’s care is more important than your own. This workshop will debunk misconceptions surrounding self-care and provide participants strategies for how to take time to nurture yourself in the midst of your busy schedule. It will be led by Heather Joy Magdelano, the founder of Journey into Joy, and mother of two children born 21 months apart with the same rare genetic syndrome and as a result both have struggled with feeding.
-
Setting Up For Feeding Success After the NICU
The Feeding Matters Workshop, “Setting Up for Success After the NICU” presented by Dr. Kay Toomey is sure to help parents, caretakers and professionals living and working with children being discharged from the NICU to be as successful of eaters as possible. Dr. Toomey discusses how very complicated feeding babies is, as well as when and why children may begin to struggle with their feedings/eating across the first 2-3 years of their lives. At each developmental time point, Dr. Toomey suggests strategies for Setting Up Your Child For Success in order to begin them on the path of developing a healthy, lifelong relationship with food.
Look for a brand new virtual workshop coming in late May 2018! In Neonatal Nutrition: Improving Short and Long-Term Outcomes, Matthew Abrams, MD will discuss interventions from the moment babies are admitted to the NICU to their nutrition after discharge to optimize growth and nutrition and long term neurodevelopmental outcomes. Although we are still in the infancy of truly understanding the complexity of nutritional components and how to best provide them to premature infants, we have reasonable data that indicates that better nutrition results in better outcomes and less morbidities short and long term.
INTRODUCING FEEDING MATTERS PROFESSIONAL COLLABORATIVE
Published by Feeding Matters on May 30, 2018
Created to transform the local systems of care in communities across the United States, Feeding Matters’ Advocacy and Early Intervention Model (AIM) brought together more than 28 community partners interested in establishing replicable norms for identification, early intervention, and healthcare reimbursement for children with pediatric feeding disorder.
Over the last 18 months, the Arizona AIM Task Force has been hard at work examining the needs of the local Arizona community and determining which of these local needs point to a greater demand from the feeding community at-large. The issues that arose during the community analysis included a lack of awareness on pediatric feeding disorder, the inability to access providers, and an inadequate pool of qualified providers.

With this in mind, the task force identified education and professional collaboration as high areas of need for the field.
To meet this need, Feeding Matters is launching its newest program – the Professional Collaborative. This mentoring program for medical professionals and clinicians in Maricopa County will feature curriculum and resources on pediatric feeding disorder, with the goal of eventually expanding the program nationally.
The Professional Collaborative aims to reduce medical risk and co-morbidities by increasing participation in meaningful life function necessary for health and wellness. This program will also reduce the economic stress of prolonged medical dependency, promote caregiver mental health, lower the risk of child neglect and injury, ensure access to high quality care, and decrease overall costs through efficient service delivery. Additional benefits from the formation of the Professional Collaborative include the following:
- Therapists will be able to utilize a local network for collaboration and expertise/advice.
- Referrals to the proper healthcare provider will be made more accurately and effectively, thereby decreasing waitlists for medically-fragile children.
- Enhanced collaboration through a highly-skilled cohort of medical professionals will enable enhanced care.
Interested in learning more about Feeding Matters Professional Collaborative? Register for our monthly healthcare professional newsletter or click here to vote on curriculum topics and submit your own ideas!
WAYS TO SERVE
Published by Feeding Matters on Jan 04, 2018
With the start of a new year, we are energized to continue our work advocating for a functional system of care for children with pediatric feeding disorder, knowing it is not possible without the ongoing support, time, and expertise of medical providers, researchers and allied healthcare professionals.
By joining forces, we are expanding educational opportunities, accelerating identification and igniting research. From professional councils to research committees, groups are coming together to generate amazing results for this misunderstood and underserved population of vulnerable infants and children. Watch this video to learn how Feeding Matters is helping healthcare professionals propel this field forward.

Monumental change isn’t easy, but with your support we are poised to create a stand-alone diagnosis for pediatric feeding disorder, screening tools, comprehensive insurance coverage, and best practices the feeding community deserves.
If you are passionate about pediatric feeding disorder, we invite you to join us in creating a world where children with pediatric feeding disorder will thrive.
Opportunities for Collaboration