Category: Healthcare Insights
Building a care team for PFD
Published by Erin Ross, PhD, CCC-SLP, CLC on Feb 26, 2024
In Washington state, every child supported by early intervention (EI) for pediatric feeding disorder (PFD) is treated by a team that includes a nurse, dietitian and a speech and language pathologist (SLP) or an occupational therapist (OT). The clinicians work together to coordinate care and discuss each child’s needs. It’s a model of care that works –– but is also extremely rare.
Many states are moving in the opposite direction for EI –– providing children ages 0-3 with services from a single provider. This may be a physical therapist (PT), OT or an SLP. That clinician is expected to cover every area of the child’s developmental therapy. Even with the best intentions, clinicians will fall short of providing the comprehensive care required for PFD.
Outside of feeding clinics and children’s hospitals, many children with PFD are treated by a patchwork of clinicians who don’t easily coordinate care. Those who seek a spot in a feeding clinic face long waiting lists and typically experience severe symptoms of PFD.
Finding support for four domains of PFD
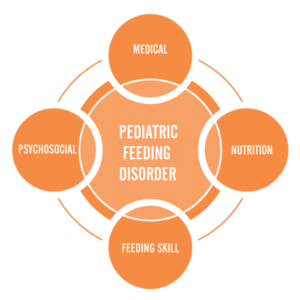
Pediatric feeding disorder affects four domains of feeding:
- Feeding skill: Actual feeding skills, such as chewing and swallowing and managing the sensory aspects of eating
- Medical: The body’s physical ability to digest food
- Psychosocial: Learned ability to eat without distress
- Nutrition: Willingness to eat a variety of foods with high nutritional value
Feeding Matters’ Coordinated Care Model examines the complexities of PFD through these four key domains that significantly impact a child’s lifelong well-being. Because PFD is so multidimensional, children need support to cover each domain. This requires a multi-disciplinary care team.
PFD can be well-regulated and treated through collaborative care and the proper support system. But for many parents, the job of cobbling together a PFD care team falls upon them.
Designing the all-star PFD care team
Symptoms of PFD vary for every child. Some common ones include a lack of interest or refusal at mealtimes, extreme picky eating and slow weight gain. If this sounds familiar, know that it’s not okay if mealtimes are a constant struggle. Unfortunately, some providers may discount these behaviors. A good rule when working with any clinician is that if you are worried, this means there’s a problem.
If you are building a care team for your child with pediatric feeding disorder, seek support from clinicians who can cover the four domains of feeding. Consider finding support from pediatric clinicians who work on telehealth if you live in an area with limited options.
Medical domain
This provider has expertise in your child’s overall medical health, such as a pediatrician, nurse practitioner or physician assistant. Their job is to identify when feeding needs additional assessment. If your child shows signs of PFD, you’ll need a provider who understands the disorder and the four domains that make up the coordinated care model.
Feeding skill domain
An OT or SLP with expertise in teaching the skill of feeding is an important member of your PFD care team. They’ll focus on the development and coordination of the sensory and movement skills that eating requires.
There’s overlap in the feeding skills and OT and an SLP can support, so be sure to describe your child’s challenges with the clinician. Ideally, you can work with both as they each bring expertise. Look for an OT and/or SLP with expertise in sensory and oral motor skills.
Psychosocial domain
Mental health providers, such as a psychologist or a licensed social worker, can help assess and treat the learned avoidance behaviors typically seen with a pediatric feeding disorder. For the child, this means managing mealtime behaviors and learned responses. This also includes modifying caregivers’ responses to the child’s behavior to promote a positive and successful feeding interaction.
Nutrition domain
It’s important to distinguish a registered dietitian (RD) from a nutritionist. In most states, individuals call themselves a nutritionist with no formal education or medical licensure association. Look for an RD with pediatric experience. Many RDs work over telehealth.
Finally and most importantly, you, as the parent, are a key member of the multidisciplinary team. You know your child best. It’s important you feel the team is listening to you and not just talking at you.
Tips for coordinating your child’s care
Ideally, your child’s care team will communicate on their own. When this doesn’t happen, serving as a middleman for provider communication is challenging. Ask your child’s clinicians to follow up with one another rather than passing messages and forms through you.
Tell the practitioner that you would really appreciate it if they would contact the other clinician. When your child is able to go to a multi-disciplinary team under one roof, that’s how they would function. Even when that’s not the case, you can still set that as the expectation for your child’s care team.
Most importantly, trust your gut. Many people are raised to think physicians are going to direct care. This is often true, but if you feel a provider is missing something or you want a second opinion, you are your child’s advocate.
If you think feeding is a problem, it’s a problem.
To find a licensed professional in your area, visit the Feeding Matters Provider Directory.
Dr. Erin Ross is a practicing SLP and the owner of Feeding Fundamentals, an organization that provides evidence-based professional training to advance the practice of infant feeding. She is a long-time member of the Feeding Matters Founding Medical Professional Council.
Getting the most out of feeding therapy for PFD: A step-by-step guide to finding the right pediatric feeding therapist
Published by Nicole Williams, OTD-OTR-L, at Desert Valley Pediatric Therapy in Arizona on Feb 15, 2024
When your child needs feeding therapy for pediatric feeding disorder (PFD), navigating the system to access treatment can be challenging. If your pediatrician recommends feeding therapy, the following are some tips for how to find the right match.
Understand the role of feeding therapistsFeeding therapy requires additional training that neither pediatric speech and language pathologists (SLP) nor occupational therapists (OT) typically learn in graduate school. Look for a clinician who has obtained this additional training and has been mentored by another experienced feeding therapist.

Both SLPs and OTs can be qualified to provide feeding therapy. There are times when one discipline is better equipped to support your child than the other.
SLPs have extensive knowledge of swallowing, chewing and the oral motor part of feeding therapy. If your main concern for your child is choking or chewing, speech therapists are best equipped to help.
An OT is an expert in sensory issues and texture aversions. If the feeling of food in your child’s mouth, combining foods or picky eating are the issues, look for support from an OT.
Even in the initial feeding therapy evaluation, you might want to request one specialty over the other. If you’re unsure, let the intake team know your feeding concerns. They should be able to match you with the right therapist.
Check your insurance benefitsIn many cases when a child needs feeding therapy, the referring physician will not indicate whether the therapist should be an SLP or an OT. In some cases, though, your insurance will specify coverage for one or the other. It’s a good idea to understand your benefits before requesting a therapy intake evaluation.
Set expectations from the startTo get the most out of feeding therapy, share your goals from the start. Even during the initial evaluation, it’s important that you and your child’s therapist have aligned goals. For example, if your child responds to a specific approach or personality, be sure to share that. In many cases, therapists can adjust to match your child’s needs. Part of the therapeutic use of self is learning to gauge and meet children where they are.
Feeding therapists have to be flexible. This means goals should be fluid from the start. If your child isn’t reaching their therapy goals, it’s time to adjust them. If your child has a setback, like a hospitalization, you may need to change your goals entirely.
Find out how to be a partner at homeAs feeding therapists, we only have one hour a week to work with a child. That’s why we typically ask parents to join us during sessions so you can continue the therapy at home. As much as parents need breaks built into the schedule, therapy is not the ideal time.
 Expect collaboration
Expect collaboration
From the start, feeding therapy is collaborative. During the initial evaluation, you’ll set goals and therapy expectations together with the therapist. You should also expect your therapist to work closely with any other clinicians who support your child.
Know that feeding therapy is not linearUnlike the progress you might see in speech therapy, for example, feeding therapy tends to progress at a slower pace. Overall, you’ll want to see an upward trajectory of progress in feeding therapy, but it’s normal for your child to have ups and downs. What you don’t want to see is a plateau over time.
Don’t be surprised if it takes time to see progress in feeding therapy. Some kids are slow to build rapport and feel comfortable with a therapist. If your therapist is answering your questions, being collaborative and is confident in their approach, be patient.
Don’t be afraid to pivot if it’s not working outIf you’re not seeing positive progress over time or if your child’s feeding therapist isn’t a good fit, be sure to raise these concerns. In many cases, the feeding therapist can make improvements.
If results don’t improve, your child may need support from another therapist. Try switching therapists to see how your child responds. If that doesn’t help, your child may need support from another discipline entirely –– such as a gastroenterologist or a psychologist.
Consider the following questions and answers for a potential feeding therapist:
Q: How long have you been seeing and treating children with pediatric feeding disorder? A: Look for someone with at least a few years of experience.
Q: Are you familiar with the Pediatric Feeding Disorder Consensus Definition and Conceptual Framework article published in the Journal of Pediatric Gastroenterology and Nutrition? A: If not, look for someone willing to read the article.

Q: Do you have specific education and training regarding pediatric feeding disorder? A: Look for someone who has additional training to understand the issues.
When therapists finish school, they usually don’t just jump into feeding therapy. Feeding is a specialty within speech therapy and occupational therapy that requires additional training and guidance under an experienced feeding therapist.
Q: Have you seen a child who’s had a similar experience?A: Finding a therapist familiar with your child’s specific feeding challenges is important. Don’t be afraid to ask this specifically to be sure you’re comfortable with the answer.
Q: Describe your overall approach to pediatric feeding disorder.A: Look for someone who understands the medical, nutrition, feeding skill and psychosocial domains and is willing to collaborate with a multidisciplinary team.
Q: How do you determine if a child is growing well? A: Look for someone who follows your child’s growth pattern, not just a standard growth chart.Q: How do you share the results of diagnostic testing, treatment goals, and other information with me and other providers treating my child? A: Look for a practitioner who partners with professionals in other disciplines and keeps open lines of communication with them as well as with you. Make sure they are willing to provide you with copies of reports and take the time to go over reports with you.
New Clinical Tool Available
Published by Feeding Matters on Dec 19, 2023
A new clinical tool has been authored by MAJ Patrick Reeves MD, FAAP.  The Clinical Action Plan for Enteral and Parenteral Nutrition is a free open access resource designed to simplify knowledge transfer on enteral and parenteral nutrition from the medical team to the child and family. These types of tools address health literacy challenges by creating a method in which to share complex information in a concise and easy to understand format.
The Clinical Action Plan for Enteral and Parenteral Nutrition is a free open access resource designed to simplify knowledge transfer on enteral and parenteral nutrition from the medical team to the child and family. These types of tools address health literacy challenges by creating a method in which to share complex information in a concise and easy to understand format.
View a FREE presentation on how to use the tool here.
Feeding questionnaire a springboard for physical therapy needs
Published by Karen Crilly, PT DPT, Advanced clinical specialist at Texas Children’s Hospital on Oct 20, 2023
How one physical therapist uses the Infant and Child Feeding Questionnaire to identify a child’s areas of need and how she can help

Feeding challenges never occur in a vacuum. While I’m neither a speech therapist or a feeding therapist, the Infant and Child Feeding Questionnaire® (ICFQ©) from Feeding Matters remains one of my most important assessment tools in my initial encounters with new patients.
The ICFQ was authored in partnership with internationally renowned thought leaders representing multiple disciplines related to feeding. It’s an age-specific tool designed to identify potential feeding concerns and facilitate discussion with all members of the child’s healthcare team – including physical therapists (PT).
Based on the caregivers’ responses to six questions, the ICFQ has been shown to accurately identify and differentiate pediatric feeding disorder (PFD) from picky eating in children 0-4.
Using the feeding questionnaire as a physical therapist
Whenever I meet with a new PT pediatric patient at Texas Children’s Hospital, I spend the first session speaking to the family to determine how we can help the whole child.
For example, I recently was working with a family in the plagiocephaly – head-shaping – clinic at Texas Children’s. When I asked the parent about feeding, she responded that the baby just won’t stay still to eat. That response led me to ask more questions about feeding. I learned the baby has torticollis – tightness of neck muscle that causes the baby to turn to one side. Plus, the baby was dysregulated, which could mean a neurological issue. I asked about reflux, which could be a gastrointestinal issue. I knew how to help in some areas as a PT, and I knew to refer the family to an occupational therapist and a speech pathologist.
I can’t even describe how relieved this parent was. When it came to feeding, everyone else had simply told her to “keep trying.”
While physical therapy focuses on a child’s functional mobility, no movement’s isolated from the rest of a child’s health. Movement takes mental and physical regulation. An infant requires proper nutrition to perform at their highest level. A child without enough calories doesn’t have the necessary energy to make the most progress in physical therapy – or any other therapy, for that matter.
6 feeding questions that help me identify physical therapy patients’ needs
There are six basic questions on the ICFQ that clinicians identify when a child has a feeding issue. As a physical therapist, responses to the questions highlight issues around endurance, function level and the parent’s understanding of the child’s needs.
Following are the six questions and how the responses help me as a physical therapist.

- Does your child let you know when he/she is hungry?
This question gives me insight into how well parents understand their child’s communication cues. Recognizing an infant’s or nonverbal child’s cues allows parents to know when a child is hungry, uncomfortable or tired. This communication is essential to the parent’s ability to do PT exercises at home.
- Do you think your baby/child eats enough?
Often, the responses to this question are cultural. Among the patients I see at Texas Children’s, I find some cultures expect babies and children to eat more than others. This is an opportunity to educate parents about what is typical. For those babies and children not getting enough nutrition, it’s a chance to refer them to specialists who can help.
- Do you have to do anything special to help your baby/child eat?
This question helps me gauge a baby’s stamina level. The baby may be having trouble coordinating breathing with swallowing. This tells me that in physical therapy, I need to work on the baby’s ability to open her chest out wide and back in. The goal is to increase the baby’s endurance to work for 30 minutes of exercise. That causes fatigue at the time, but it actually builds stamina for later.
A baby who doesn’t have the endurance to finish feeding isn’t likely to have the energy to make as much progress in physical therapy. This makes getting more calories into the baby especially relevant for PT.

- Do you have to do anything special to help your baby/child eat?
This question helps me determine when a baby is dysregulated. It means I need to refer to a specialist who can help the family uncover why feeding isn’t typical.
In physical therapy, I’ll determine whether the child needs to work on muscle retraction. This is one of the issues I see often in infants, especially, and sometimes even older children who are having trouble feeding. Retraction takes them away from their midline without being able to find their center again easily. This makes it difficult to eat.
As a physical therapist, I’ll work with the baby on midline rotation. We work on coordinating the movement of opening and closing the arms and chest. The baby’s shoulders should expand back and then be able to come back to center. The baby should be able to find his flexion and make symmetrical motions in the upper and lower body.
Working on the body in this way can improve feeding, supporting the therapy that speech pathologists and occupational therapists are doing as well.
- Does your baby/child let you know when he is full?
When a baby is not recognizing fullness, this indicates there might be a chronic condition. Once full, a baby should cry, turn the head, push away the breast or bottle or spit out milk. But if a baby just keeps eating, this is a cue that the family needs a referral to a specialist.
As a physical therapist, it helps me identify a baby’s level of function.

- Based on the questions above, do you have concerns about your baby/child’s feeding?
Responses to this final question provide an opportunity for education. I’ll know how much information I should give parents on typical development for their child’s age and stage.
It’s also an opportunity to encourage parents who need a referral to go ahead and make that appointment.
As physical therapists, we’re not just looking at the legs and the feet. Treating our patients means treating the whole patient.
Knowing how a child is feeding doesn’t only alert me to a patient’s nutrition needs. It helps me identify other issues a child might be experiencing. Each question in the ICFQ paints a picture of the whole child’s needs.
Karen Crilly, PT, DPT, MAPT, CBIS, is an advanced clinical specialist at Texas Children’s Hospital who has dedicated her professional life to forming a strong background and expertise in the assessment and treatment of infants and children with chronic and complex developmental and/or neuro-motor impairment.
Supporting a smoother transition to home for NICU babies
Published by Feeding Matters on Oct 02, 2023
In his years as a neonatologist, Vincent C. Smith, MD, MPH, has found anecdotally and in his research that the clinician managing a family’s discharge from neonatal intensive care units (NICU) disproportionately impacts patient outcomes.
Smith, the division chief of newborn medicine at Boston Medical Center, led a study examining how families are prepared for discharge and found significant variability in outcomes. Families with a primary nurse invested in their transition home after NICU discharge fared better. “It wasn’t about gestational age, length of stay or medical complexity. That discharge clinician sets the course,” he says.
Smith wasn’t alone in his findings.
Clinicians across disciplines working with NICU families, as well as parents, find that whether families are ready for the dramatic adjustment of going from a team of clinical support to being on their own is usually left to chance.
Erika Goyer, parent liaison and communications director of National Perinatal Association (NPA), says, “Medical care is siloed. You have a high-risk pregnancy with one team. Once your baby is born and needs intensive care, they’re transferred to the NICU, and you move on to another team. As your baby progresses, you’re supposed to move on to a team at home. What that team comes down to at home is usually just you.”
An estimated 9-13% of newborns in the U.S. require neonatal intensive care for complex medical needs, a number that’s increasing.
To support these families, a cohort of multidisciplinary clinical leaders – including Feeding Matters – and parents came together to standardize NICU discharge. Their hope with the NICU guidelines is to improve families’ experience, reduce stress and help NICU babies access the follow-up care they need to thrive.

Why NICU families need more support
If you speak to NICU families after their first night home, says Smith, what’s true for all of them is that none slept comfortably. Even in the best circumstances, there tends to be a lack of continuity for families. “A lot of families feel abandoned by the NICU. They get their papers and their baby, and they’re joyous. Then they go from bells, whistles and lights, with 50 people around to just them and a baby. And they just had to make do.”
Kristy Love, executive director of NPA and NICU patient advocate, knows firsthand what it’s like to have a child in the NICU. Both of her children were NICU babies. She spent as long as three months in the hospital with one of her kids. What she’s found in her years supporting other parents is that not much has changed since she struggled to transition home with her preemie over 20 years ago. Parents still contact her as much as a year after leaving the NICU to share their struggles. “We have all this support in the NICU during our journey, and then once we go home we’re flying solo,” she says.
She shared her concerns with Smith at a board meeting for the National Perinatal Association, and from there, the NICU discharge guidelines were born.
NICU discharge guidelines explained
The National Perinatal Association spent a year looking at NICU discharge factors like research, protocols, insurance benefits and parents’ experience. The National Perinatal Association looked at NICU discharge factors like research, protocols, insurance benefits and parents’ experience. They worked together with a group of multidisciplinary experts, including Cuyler Romeo MOT, OTR/L, SCFES, IBCLC, director of strategic initiatives at Feeding Matters. Together the content experts finalized the NICU guidelines and submitted them to the Journal of Parentology for peer review.
The guidelines address topics like:
- Basic information
- Anticipatory guidance
- Family and home needs assessment
- Transfer and coordination of care
- Other important considerations
Smith says there are around 300 guidelines, and no one expects NICUs to adopt all of them at the same time. The hope is that hospital neonatal teams will identify a few of the guidelines particular to their organization and population and then build from there. Over time, they can gradually implement all of the guidelines.

“Many people get overwhelmed when they see the challenges before them because they don’t necessarily have the team, resources or funding. I find everybody can make small changes leading to bigger changes,” says Smith.
Having peer-reviewed guidelines is an important step to improve all families’ experiences. Organizations like the American Academy of Pediatrics and others recommend that hospitals have a transition plan, but it was never formalized until now. “Everybody said you needed to have a plan in place to execute, but they weren’t given any guidance on it,” says Goyer.
Pilot program to put NICU guidelines into practice
Having NICU discharge guidelines is an important first step. Putting it into practice in the field is essential. When the team who wrote the guidelines looked for a NICU as a pilot program for implementing them, they chose Banner-University Medical Center Tucson.
Romeo, who served on the guidelines committee, is a clinician there. Plus, a local community partner, Smooth Way Home, helps families transition home from the NICU.
In January 2022, Romeo says they launched the pilot program by identifying barriers to a smooth transition home. Through crowdsourcing in the unit and close collaboration with the developmental RNs, Nancy Gates and Ashley Lee, they chose three areas of focus:
- Processes: Discharge processes and coordination
- Providers: Community provider readiness to accept infants into community-based care
- Parents: Parent and caregiver education and advocacy to support optimal care and development at home
The team found that families may not receive developmental care support once they were discharged home. It was unclear if families referred to the Arizona Early Intervention Program (AzIEP) were receiving care. Not all children discharged from the NICU qualify for early intervention services despite their difficult beginnings. If they did qualify, getting that first appointment proved challenging. “Before piloting the guidelines, our NICU team would refer families to AzIEP and then have no way to know if they received care,” says Romeo.
A long standing barrier to accessing services after discharge was knowledge sharing. Nancy and Ashley reported that early intervention agencies often were unable to access the infants’ medical records. Without this information it was difficult for families to qualify for service.
To address these issues, says Romeo, the developmental RNs are leading the way in investigating process improvements for information transition while working closely with Smooth Way Home as a liaison for a warm handoff into the EI system.
It’s a multi-year pilot program that we hope will grow into a larger program if we are able to secure funding. Our families deserve to be well prepared so they can finally enjoy their baby at home.
Romeo says the guidelines lead to better outcomes, but funding remains the most significant barrier. “This work is done while the clinicians continue to fulfill their typical job demands. Nancy and Ashley do not have time allocated for this project, but they feel it is vital to the infant’s health and development so the work continues.”
 Everyone involved says improving the continuum of care for NICU babies and their families requires tremendous work. But every level of improvement matters to the families who benefit from it. As Goyer says, “This is all about making sure families aren’t alone and have the support and skills they need from the clinicians and community around them.”
Everyone involved says improving the continuum of care for NICU babies and their families requires tremendous work. But every level of improvement matters to the families who benefit from it. As Goyer says, “This is all about making sure families aren’t alone and have the support and skills they need from the clinicians and community around them.”
Visit NICU to Home for more information about the NICU guidelines. Feeding Matters has been a strategic partner in creating and implementing the guidelines, together with NPA. For more information about how we help families of children with pediatric feeding disorder, click here.
Focus on Food Safety
Published by Anna Busenburg, RD, CSP, LD, CLC on Sep 05, 2023
This blog post is published as part of a paid partnership between Feeding Matters and Reckitt Mead Johnson Nutrition. Learn more about our corporate partnership program and ethical standards for collaboration.
There are many opinions on using human milk or infant formula when it comes to feeding your baby. Most of the focus goes into what is being fed to your child, but less emphasis is placed on the safety of how feedings are prepared. Unless you are directly breastfeeding your child, you need to consider food safety when preparing infant bottles or tube feedings.
This focus on food safety has been front and center over the last couple of years since infant formula recalls have been in the news. These recalls occurred due to microorganism contamination concerns in a manufacturing facility. Food safety matters and is why liquid ready-to-feed or concentrated formulas undergo a heat treatment that sterilizes the product. Powder formulas are not sterilized, which poses an additional risk for contamination when incorrectly handled and prepared. The Food and Drug Administration (FDA) is the regulatory and enforcement authority over the manufacturing and distributing of infant and pediatric formulas. It is important to consider food safety when preparing both infant formula (< 12 months old) and pediatric formulas (> 12 months old) being fed via a bottle or a feeding tube.
For families preparing pediatric feedings at home, it is important to remember these safety tips:
- properly wash your hands
- clean/sanitize feeding equipment and preparation space
- store prepared feedings appropriately
- follow the recipe from your provider
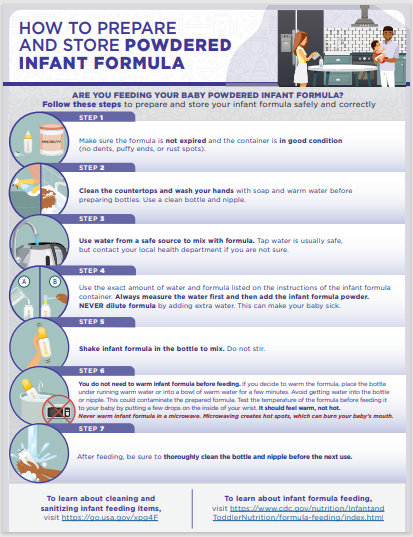
Practicing good hand washing techniques helps to diminish the risk of transmitting germs. Make sure that hands are washed for a full 20 seconds with soap and water. Proper handwashing is the #1 method of preventing the spread of germs for your child.
When bottles or pump parts are being used, cleaning them regularly is essential. It is also recommended to sterilize these components in the microwave or dishwasher. Any child that has complex medical conditions has increased susceptibility to infection. Steps to clean and sterilize equipment are crucial for these children’s overall health.
Any time you mix up formula – those feedings are good to use for 24 hours. Make sure that you label and note of when feedings are mixed and store in the refrigerator until it is time for the feeding. This includes recipes of human milk fortified with formula or formula only recipes. When warming infant feedings, never microwave. Options for warming include a bottle warmer or placing bottle in a warm water bath. When leaving the house with infant feedings, transport in a cooler with ice pack to help ensure the milk/water is kept cold to decrease risk of microbial growth.
When preparing your child’s feedings, follow the recipe on the can or given by your health care provider and check the expiration data prior to preparing. Some children need special feeding recipes to meet their growth goals. Use the scoop in the formula container or measuring utensil provided by your health care provider. Use a safe water source for mixing feedings, this can be tap water or nursery water.
Feeding your child seems like the most basic parenting task, but it can be challenging and complicated for many families. Remembering some of these guidelines of food safety can help ensure that you are doing the best for your child and keeping them safe. Click here to download and print handout from the Center for Disease Control and Prevention (CDC) our HOW TO PREPARE (cdc.gov)
References:
1. Green Corkins, K., & Shurley, T. (2016). What’s in the Bottle? A Review of Infant Formulas. Nutrition in Clinical Practice, 31(6), 723–729. https://doi.org/10.1177/0884533616669362
2. Turck, D. (2012). Safety Aspects in Preparation and Handling of Infant Food. Annals of Nutrition and Metabolism, 60(3), 211–214. https://doi.org/10.1159/000338215
3. Green Corkins, K., & Shurley, T. (2016). What’s in the Bottle? A Review of Infant Formulas. Nutrition in Clinical Practice, 31(6), 723–729. https://doi.org/10.1177/0884533616669362
4. CDC. (2018, May 7). Infant Formula Preparation and Storage. Centers for Disease Control and Prevention. https://www.cdc.gov/nutrition/infantandtoddlernutrition/formula-feeding/infant-formula-preparation-and-storage.html Accessed August 8th, 2023.
Anna Busenburg, RD, CSP, LD, CLC has been a registered dietitian for the past 11 years and specializes in pediatric nutrition and specifically neonatal nutrition, working in a level IV NICU at Cincinnati Children’s Hospital Medical Center. She has covered inpatient NICU and outpatient NICU follow-up clinic patients.
She has undertaken many projects over the years to help improve patient care and cultivate a culture to support nutrition education. She has been involved in developing a process for utilizing donor breast milk in a 25-bed NICU and she was involved with leading the launch of a breast milk/formula scanning system in a 100-bed NICU. Anna is a certified specialist in pediatrics and has completed the pediatric weight management course. She obtained her Certified Lactation Counselor credential in 2019.
She authored a chapter of the book The Nutrition Communications Guide from AND published in 2020 and published an article in the Pediatric Nutrition Practice Group on RDs Involvement in Infant Feeding Preparation Rooms published in 2019. She currently serves on multiple committees for the Pediatric Nutrition Practice Group and has held various positions within AND on the state and local level. She is also a member of the American Society of Parenteral and Enteral Nutrition. When not busy with work, Anna spends her extra time and energy with her family, which includes her husband, 3 boys, and a Chihuahua.
Pediatric feeding with empathy: 8 ways to think through a compassionate lens
Published by Marsha Dunn Klein, pediatric occupational therapist on Aug 17, 2023
On a vacation to Monterey, Mexico, I sat at a fancy restaurant and friends presented me with a plate of worms. Since I am a curious eater, and it was a delicacy, I cautiously took a bite.
At that moment, I couldn’t help but think of my feeding therapy clients. After decades as a pediatric occupational therapist, I wondered, “If somebody made you eat this, held your hands down while they put it in your mouth, or made you eat three bites of those worms before you could have your regular dinner, would that be fair?”
Understanding how children feel during mealtime is the pediatric feeding with empathy that I try to share in my teachings with parents and feeding therapists. Empathizing with why children struggle to eat or drink is key to setting clients up for a lifetime of better feeding. “We need to look deeper to find a compassionate lens. The foundation for supporting all areas of feeding therapy has to be fully cemented in an understanding of empathy, connection, safety, motivation, enjoyment and brain science.”
In a presentation at the International PFD Conference, I outlined eight mindset shifts to consider for a more empathetic approach to PFD feeding therapy.
Communicate the empathy circle
Empathy is the ability to understand and share the feelings of another. It’s the ability to sense another’s emotion and imagine walking in their shoes. For children and their parents, pediatric feeding with empathy means seeing food as they see it and reflecting to them that they’ve been understood.
Communicating what might be going on for a parent or the child is called the empathy circle. We need to find empathy for the child and what they might be going through. And we need to help parents have empathy for their child and understand what might be going on for them.
Look beyond just calories during mealtime
Nourishing children needs to include more than focusing on calories. Having a child feel like a celebrated part of mealtime is essential to skill mastery. Food is nourishment, but it’s also a means of communication and socialization. It can be about giving and receiving love, celebration and family time. This is why mealtime is an important opportunity to develop strong parent-and-child relationships. We need to ensure we’re also nourishing little souls with pleasant, safe company.
Shifting adult and child roles during meals
The role of adults at mealtime is to decide the menu and provide a safe environment for learning. When children come to the table, it’s to be nourished and have energy for the day. That means some of the foods offered at that mealtime must be foods the child knows and will comfortably eat while they’re learning about other foods that the family and siblings are eating.
Many of us have approached feeding therapy as if it’s our job to “get food into kids.” However, it’s the child’s job to decide what and if they’re going to put food in their mouths, and our job is to offer a variety of foods to allow for opportunity and learning about foods so the child can discover what he LOVES.
Rethink exposure to new foods
In the past, exposure to new foods meant getting a child to put it in their mouth. In some cases, a child gets pushed past their sensory safety zone. Exposure done with pressure can decrease the enjoyment of eating, along with any benefits of that exposure.
Asking a child with PFD to try a mouthful may be way too big of an ask. A little taste, lick, touch or even seeing others enjoy a food can be considered an “exposure.” Instead of thinking of “exposure” where adults often ask (or demand) that children interact with that food in a certain way, can we think of “opportunity” where the child gets to explore the food and decide if or when ready to try it on their own.

Work with the whole family
Both parents and children bring their experiences to the table. A trusted connection with parents from infancy supports a child’s ability to self-regulate. Feeding therapists must be sure to support parents’ success. This means asking assessment questions that reflect what’s going on with a child and parent. It also means including parents in planning and solutions with questions like: Of all the things we did today or talked about today, what would you like to try this week?
Consider why a child says no
A child says no to food for a reason, such as:
- They don’t feel well
- The sensory challenge is too great
- They have a difficult motor response to that food
- They have poor regulation
- They are too worried
Consider food refusal as communication. It invites us to be curious about what’s going on and how we can make that child feel more ready and safe for this mealtime interaction.

Shift from food tolerance to enjoyment
Tolerance is the capacity to endure pain or hardship. But enjoyment means satisfaction, pleasure and gratification. Food constitutes not only the taste but also sensory aspects, socialization, experience and satiation. Many of us have used the word “tolerance” in our feeding goals. But if a child doesn’t like that food, why would we settle for “tolerance” when we could aim for “enjoyment?”
Pay attention to communication cues
Forcing a child to eat when the adult is the more powerful figure in the relationship could mean missing cues of a child’s sense of safety, worries and need to protect themselves. It’s easy to push into their stress and worry zone and then call food refusal a behavior problem. This can unintentionally teach a child to ignore their body and sensory cues.
When we allow children to tune in to the wisdom of their own bodies, we’re supporting safety. Children who experience safety with us as parents and therapists are better able to regulate themselves. Pediatric feeding with empathy means seeing them, hearing them, valuing them and understanding them, to climb into their skin and walk around in it.
Ultimately, eating is a learned behavior. How parents and children interact over mealtimes matters. This is why parents and feeding therapists must do what they can to create positive memories around eating, food and mealtimes.
View Marsha’s International Pediatric Feeding Disorder Conference Session: Shifting our Focus in Pediatric Feeding Towards a Compassionate Lens here
Marsha Dunn Klein has spent over five decades working in feeding therapy as an occupational therapist, author, inventor and co-founder of the Get Permission Institute. This article is based on a presentation from the 2023 Feeding Matters International Conference.
My Experience Researching PFD
Published by Michelle McKay on Aug 08, 2023

Hello! I’m Michelle, and I am thrilled to share where my inspiration for becoming a feeding therapist came from and introduce my newest research project. I have a full-circle story of how I ended up working in the field of pediatric feeding. I am so passionate about working with these clients and their families.
When I was a junior in high school, a friend asked if I could help her babysit for a family in my neighborhood. I became this child’s habilitation and respite provider and began attending their therapy sessions. I loved all of them, but was particularly intrigued by his feeding therapy sessions. I started helping with his home program, introducing new foods, playing with new foods, and working on feeding skills at home. I knew that was the space that I wanted to be in when I grew up, and I worked hard to graduate with my doctorate in occupational therapy in 2020.
During my capstone in my OT program, I began a small research study, studying the interventions I was observing in feeding therapy. Unfortunately, in the middle of this experience, the COVID-19 pandemic hit, and I was unable to get my study off the ground.
I have always been a question-asker and answer-seeker, looking to research and clinicians with more experience for advice and support for how to best help my clients and their families. Since graduate school, I have been interested in returning to my research question and helping feeding therapists provide the most evidence-based interventions to support our clients and their families.
As a therapist, I get my evidence and best-practice by learning from families, colleagues, and reading the most current research. However, with pediatric feeding disorder as a new diagnosis and feeding therapy as an emerging practice area, research on feeding therapy interventions is scarce. This is the gap I’m trying to address as I begin my journey into conducting research.
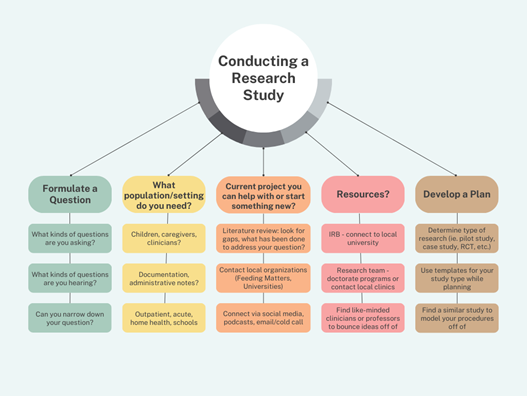
- Formulate a question. What are common questions that you find yourself asking or that you are asked by families, other practitioners, or from people that you are mentoring? For me, I was often asking why are these the interventions that I keep coming back to. I ask myself daily how the strategies that I choose to use are helping my clients find success at mealtimes. I have asked the same questions of all of my mentors and frequently find caregivers or other health care providers asking the purpose of certain strategies that I bring to the table.
- What population/setting do you need? Could you answer your question using the data from your documentation? Do you need to study your clients or their caregivers or other clinicians? Where would you find data to support your research? Would you need to be in an outpatient clinic, a hospital or acute care setting, home health, school, etc.?
- Current project you can help with or start something new: Are there current research projects that are addressing your question or a question you’re interested in, or do you need to start your own? Start with a literature review to look for what’s been researched and where the gaps are. Contact organizations or communities that may be doing research (ie. Feeding Matters, Universities, etc.). Use social media to find others who are like-minded and connect with them. Don’t be afraid to send a DM or email to a researcher or clinician who you relate to who may be interested in helping with your idea.
- Resources: If you’ll be conducting research with human subjects, you will need an IRB. The best way to get an IRB is to connect with a university. Doctorate programs in the therapy fields are becoming more common and often have benefits for community research partners including access to student research teams, access to university libraries and libraries who can help with research design, and professors who may have similar interests or projects that you can model yours off of.
- Develop a plan. Through your literature search, determine which type of research fits your question and resources best. Will you be conducting qualitative or quantitative data? Do you have the resources and ability to pursue a randomized control trial, or would a pilot study or case study fit better? Take time to find the right research type for you. Use templates for research protocols, plans, and write-ups from the beginning that match your study type, especially if this is the first study you’re leading. During your literature review, look for strategies in their research protocols that you can model your procedures off of and save these ideas together to reference as you work on yours.

A mother’s journey with PFD shines a light on research
Published by By Hayley Estrem, PhD, RN, Assistant professor at UNCW on Jul 21, 2023
I clearly remember the day a doctor’s news changed my life. After months of chasing my baby around with a bottle to eat an ounce at a time, I learned Alex has a rare chromosome disorder.
The neurologist enthusiastically delivered the devastating news, charmed that he was the first to solve the puzzle of why Alex’s development was delayed. Even as a registered nurse, I found his explanation confusing. My shock meant I couldn’t have processed the information even if it had been simple.
How NOT to support families with pediatric feeding disorder

As a healthcare professional, that day was one of many where I learned how not to support a family of children with pediatric feeding disorder (PFD). The news should have come from a genetic counselor, my husband should have been there, and it should have been shared with compassion.
The journey before learning about Alex’s disorder was a struggle as well. Although he was my first, I knew it wasn’t normal for a newborn to eat only an ounce at a time. What he took in, he spat up. His growth was slow, and at 9 months, he was neither sitting up nor crawling.
Our pediatrician told us to give it time, that I was a nervous new mom and that Alex was slow to grow because it was a difficult pregnancy, and he would catch-up. It wasn’t until we saw a different provider at 9 months that we were connected to a neurologist, geneticist and Early Intervention (EI) services. This too, was a lesson in how not to support families of children with PFD.
Armed with a diagnosis and therapy services, we hoped to help Alex eat more and get the calories he needed to grow and develop. Instead, we were told to try harder to feed him and to schedule weekly weigh-ins. A feeding tube was held over our heads like a threat, as if inserting one would signal our failure as parents.

By the time Alex was 18 months and weighing only 16 pounds, I nearly begged for a G-tube. When he finally got one and started gaining weight, I couldn’t help but wonder why we were encouraged to try so hard. Why didn’t he have the nutrition he needed during such a critical developmental time?
Alex’s genetic diagnosis and the PFD that came with it became a springboard for my career. I had a choice to struggle with the question, “Why me?” or do something that would make this odyssey less painful for others.
I chose the latter.
Leading research to support families of children with PFD
After completing a master’s degree in nursing education and then a doctorate in nursing, today I research PFD and how it affects the entire family unit. I’m dedicated to fixing what we went through for others.
At the beginning of Alex’s diagnosis 15 years ago, there wasn’t common terminology among physicians and clinicians. This was a focus for my dissertation because it is a big barrier to building research and supporting families of children with PFD.
It’s why I have a big affinity for Feeding Matters, who did the work to get a PFD ICD-10 diagnosis.

One of the things I’ve done with our Feeding Flock Team is to develop several parent questionnaires about feeding behavior, skill, family management of feeding, and parent and family impact of feeding. For example, on a project with researchers and clinicians at Children’s Hospital of Atlanta, we are developing an assessment of the impact of intense food allergy regiments on caregivers and households.
Our goal is to provide data to clinicians and parents to help determine whether a food allergy intervention eases the psychosocial impact that food allergy has on everyday life for parents and families. For example, new oral immunotherapy treatments for food allergies require children to take a certain amount of allergenic food and have activity restrictions every day at a specific time. Is the cost-benefit worth it? Ultimately, the child still needs to avoid the food, but should have less severe reactions if exposed to small amounts unintentionally. Are there quality of life improvements for the family? We only know if we measure this.
I’ve interviewed parents as I go through the process of developing measurement tools for PFD, and I’ve heard their stories. Witnessing what others go through and being in the position to do something about it is what gives our family’s struggle meaning.
Because of our experience with feeding therapies, I learned to ask more questions. And I learned that research for PFD must be patient-centered. Only with patients who have experienced PFD and their families at the helm can research lead to better journeys and improved outcomes for the whole family.

When ‘Expert’ Advice Is Unhelpful: A Guide to Avoiding Misleading Social Media Advice on PFD
Published by Feeding Matters on Jul 17, 2023
The pitfalls of unhelpful and misleading social media advice for clinicians and caregivers and how to avoid them
Whether you’re a clinician or a caregiver, unhelpful and inaccurate content is a common pitfall for anyone following feeding therapy accounts on social media. Here’s an example that speech therapist Bri Miluk, MS, MS, CCC-SLP, CLC, owner of Pediatric Feeding Therapy, sees often.
 A therapist with a few years of experience shares a Reel highlighting the “dangers” of using a sippy cup. With a flashy video and a viral song, the account owner warns the audience of all the negative ways a sippy cup can affect speech, feeding, swallowing and sleep. Then, instead of sippy cups, the post recommends a special straw or open cup. The author shares a link to where you can buy it and the hashtag “#ad” as well.
A therapist with a few years of experience shares a Reel highlighting the “dangers” of using a sippy cup. With a flashy video and a viral song, the account owner warns the audience of all the negative ways a sippy cup can affect speech, feeding, swallowing and sleep. Then, instead of sippy cups, the post recommends a special straw or open cup. The author shares a link to where you can buy it and the hashtag “#ad” as well.
Not only is the information, at best, misleading, and, at worst, entirely inaccurate, but it also violates Federal Trade Commision (FTC) rules for advertising.
Miluk, who is pursuing a PhD in communication and information sciences through the University of Alabama, explains, “This kind of content uses fear-mongering to convince people to avoid something based on baseless claims.” Pointing out that there’s no evidence to show that a child using a sippy cup is going to have sleep, airway, feeding or speech difficulties, she goes on to say, “A sippy cup uses similar oral motor patterns as sucking on a pacifier, thumb or bottle, but we know that frequency and duration matter. A child doesn’t have a sippy cup in their mouth all day long.”
Social media is a powerful tool for education and community among caregivers and clinicians alike. But the onus is on the user to ensure the information obtained there is accurate and helpful.
Healthcare misinformation mixed with fear-mongering on social media makes a recipe for disaster
Richard Noel, MD
, a pediatric gastroenterologist at Duke Health, has treated hundreds of patients with pediatric feeding disorder (PFD) and other pediatric GI issues. One problem he hears from caregivers gathering PFD information from social media is that content typically features only one perspective. “On social media, you only see the numerator but never see the denominator. You’re not told about when an approach fails. They always generally talk about their successes.”When information is shared as a general recommendation, it can be particularly challenging. “Pediatric feeding disorder can have many different forms and severities. What works for one person may not work for another,” says Dr. Noel.
Knowing that social media can be full of inaccurate information and even fear-mongering has led clinicians like Miluk to spend time creating social media educational content. Miluk has built up an audience of over 24K on Instagram with content to educate clinicians about feeding therapy. Caregivers also follow her for tips, and Miluk is especially driven to dispel myths for both audiences.
Here’s a great example of how Miluk does this:
https://www.instagram.com/p/CuQO6cCOd-S/Clinicians need to gauge content on misleading social media advice
Even clinicians and students pursuing a therapy degree can fall prey to misinformation on social media. Miluk started sharing social media content, primarily on Instagram, after seeing other speech therapists promote inaccurate or misleading content. She started in 2020 by sharing evidence-based content on pediatric feeding. That evolved to trying to support clinicians and caregivers to better understand dark marketing and how misinformation is shared online. According to Business Review at Berkeley, dark marketing is highly targeted advertising that “causes the audience to think about the product more subtly.”
TikTok posts and Instagram Reels from influencers promoting a product take dark marketing to a new level. “Some of these sources are selling a method or a booklet, and you’re getting advertising disguised as a documentary,” warns Dr. Noel.
Because dark marketing is so pervasive on social media, Miluk teaches her students in university courses and clinicians online how to spot it.
“The better understanding we have of how to be informed consumers ultimately leads to better patient care,” she says.
Judging the accuracy of information on social media
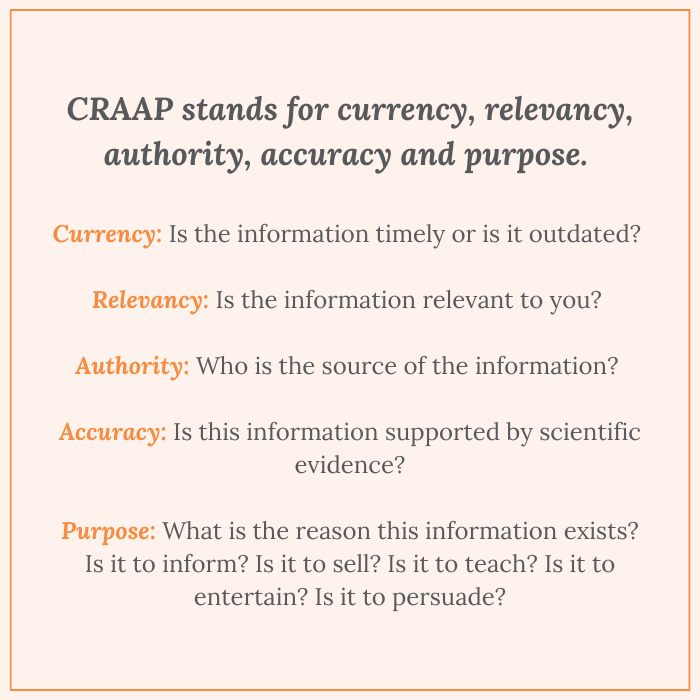
When using social media to view healthcare information, one tool Miluk recommends considering is the aptly-named CRAAP test.
CRAAP
stands for currency, relevancy, authority, accuracy and purpose. Miluk explains each letter of the acronym as follows:Currency: Is the information timely or is it outdated?
Relevancy: Is the information relevant to you?
Authority: Who is the source of the information?
Accuracy: Is this information supported by scientific evidence?
Purpose: What is the reason this information exists? Is it to inform? Is it to sell? Is it to teach? Is it to entertain? Is it to persuade?
Best practices for clinicians using social media for pediatric feeding disorder information
Miluk and Dr. Noel recommend the following ways to access informative PFD content on social media without being misled.
Just because it’s a common refrain doesn’t make it gospelOne of Miluk’s favorite podcasts, Duped by Dr. Michelle Mazur and Maggie Patterson, has a quote she repeats often: Just because you hear something frequently doesn’t mean it’s true.
“Because of cognitive biases, when we see something repeatedly, it’s natural for our brains to believe it to be true. In reality, that doesn’t mean truthfulness,” says Miluk.
Make your intentions clearFor clinicians who promote products on social media, you need to disclose any affiliations in the post. This can’t be simply including #ad. You must clearly state that you may receive a commission on qualifying purchases. “It’s something that I wish would be normalized. An affiliation is not something to be embarrassed about. People have a right to know if you have a potential bias for something when you’re earning a profit, no matter how small,” says Miluk.
Clear disclosure on posts is required by social media channels themselves, as well as the Federal Trade Commission.
Unfollow toxic accountsFor those clinicians and caregivers who actively share on social media, one of the biggest challenges is the ability to hide behind a screen. This can create divisiveness and even be shame-inducing. “If you put something on a public forum, you should expect public replies and even public criticism, but that doesn’t mean we should be disrespectful,” Miluk says.
Miluk recommends treating your social media like your digital home. “If I wouldn’t allow someone to walk through my door and talk to me like that. Then they’re not welcome here, either.”
Advice for parents and caregivers
Caregivers should be wary of social media before adopting a new method or following advice to support children with PFD. Dr. Noel recommends the following tips:
Use your therapy provider as a sounding boardWhen you find new health information, bring it to your therapy provider before investing time or money into a specific method, book or video series. “You see something new on social media that looks amazing and promises to help 10 out of 10 kids with a feeding disorder. If you run it by your therapy provider, they might point out it’s not new. It works for some, but it doesn’t work for all. That’s how you get better, more realistic information for your child,” he says.
Seek information and support from advocacy organizationsDr. Noel is a fan of and a critical professional leader for advocacy organizations like Feeding Matters. He says, as a physician, there are many questions he can’t answer because he doesn’t live with the disorder his patients’ families confront every day. Having a peer referral source is crucial. “These advocacy organizations are incredibly valuable to provide for patients’ needs that are way beyond what I do in medicine,” he says.
Technology today is moving faster than your finger can drag down to refresh. Access to this information overload is only as beneficial as the receiver’s level of skepticism. Miluk’s most important advice for using social media to find support for PFD or any other health issue is to slow down. “You have to slow down your thinking and be willing to appraise the information before feeding education on social media can be effective.”
Click here to read a blog
by Miluk on why she recommends clinicians attend Feeding Matter’s annual PFD conference.